It’s been a half-dozen years since Washington’s heated, largely “closed-door” Congressional and White House debates over “Healthcare Reform,” with close to 20 million more Americans obtaining “health insurance coverage” through the enactment of the “Affordable Care & Patient Protection Act of 2010” (also either affectionately or derisively termed as “Obamacare” depending on whose perspective you get!).
On the whole, Obamacare has delivered on mitigating some the punitive business practices of FOR-PROFIT/Big Health Insurance carriers (in the areas of widespread “DENIALS OF MEDICAL CLAIMS” or simple “RESCISSIONS/POLICY CANCELLATIONS” of some “at-risk, unhealthy” consumers’ health coverage, but the “structural foundations” of “antitrust-exempt,” monopoly-based Big Health Insurance have remained intact for 71 years and running. However, the unrelenting obsession with “gross profit exploitation,” loopholes in providing consistent/quality coverage, and “shifting of the out-of-pocket payment burdens onto consumers’ backs” with higher CO-PAYS and DEDUCTIBLES onto the backs of “policy holders” is still OVERBURDENING an already stretched-thin American citizenry and our economy as a whole.
That’s why, a half-dozen years later, I have again become determined and inspired by U.S. Democratic presidential candidate Sen. Bernie Sanders’ (I-VT) central platform of proposing a single payer-based “Medicare For All” universal healthcare system starting in 2017. This bold proposal, previously advocated by “Single-Payer” advocates and a government-funded “Public Option” advocacy effort were both BLOCKED from the “closed-door” nature of Healthcare Reform hearings held in Congress and the White House.
Since one of the core thrusts of “Obamacare” meant a broad expansion of Medicaid (for the 65-and-under years of age population) while switching some funding out for some minor cutbacks in Medicare (in place for 65-and-over Senior population since its enactment in 1966), it just seems logical and operationally practical for Senator Bernie Sander’s plan calling for an UNIFIED “Medicare For All,” single-payer healthcare system to cover the ENTIRE population of U.S. citizens.
However, getting to this “justified,” ultimate end-game for a national “Universal Healthcare” system is rife with the structural and economic challenges presented by “FOR-PROFIT,” Wall Street-based marketplace forces long artificially manipulating pricing and other kinds of “MONOPOLISTIC” business practices has to be CONFRONTED and MITIGATED to large extent – because at $3.3 TRILLION national price tag for healthcare (or roughly 17% of U.S. GDP today) America continues to spiral out-of-control as easily the most expensive healthcare “patchwork” marketplace in the world!
Those had been the kind of “marketplace drivers” which prompted me seven years ago to take on an advocacy position for “Nonprofit Community Health Plans,” which has quietly but steadily been a feature of American healthcare since this country’s colonization in the late 1600s. However, since the turn of the 20th century, when America’s economy largely steered away from both Nonprofit Community Health Plans and Ecumenical/Nonprofit-based Healthcare, ˆWall Street “marketplace forces” injected “profit exploitation-based” business models as more and more of America’s health insurance coverage and hospitals shifted dramatically into being “publicly-traded companies” dedicated to serving large institutional shareholders/investors demanding higher and higher revenues, earnings and profits in our century-old “Capitalist-dominated” healthcare marketplaces.
Originally, I had formed an activist organization called “Americans for Non-Profit Health Insurance Exchanges” (ANPHIE) to advocate those “Nonprofit Community Health Plans” (operating in most of America’s 50 states of the Union). But after “Obamacare” was officially implemented in stages starting in 2011, so-called “state-run health exchanges” allowed some of the nonprofit health plans into their exchanges. However, those state-run exchanges continue to be dominated by “FOR-PROFIT/Big Healthcare Insurance” carriers, which are still granted “antitrust-exempt monopolies” because of the 71-year-old McCarron-Ferguson Act of 1945 essentially allowing the federal government to “abrogate” all oversight and responsibilities for the states to determine oversight and enforcement.
Unfortunately, most state “Insurance Commissions” typically feature “former For-Profit/Big Health Insurance executives” who dominate state boards over what could be said is the most LAX oversight that could ever be imagined for BILLIONS of Americans unnecessarily SUFFERING and DYING because of a “monopoly-based, exclusionary FOR-PROFIT/Big Health Insurance marketplaces for the last eight decades.
Up to today, NOTHING much has changed with the basic “underlying marketplace fundamentals” of artificially-inflated and manipulated pricing, anticompetitive market-share coercion and collusion, the continued burden shifting onto consumers of higher “co-pay” and “deductible” requirements, and a renewed effort by FOR-PROFIT/Big Health Insurance carriers to arbitrarily review certain “experimental” medical procedures for DENIALS of certain claims. White it is true that maybe 19 million more Americans have coverage under “Obamacare,” they and about 30 million remaining uninsured or underinsured Americans continue to be subject to America’s “Have or Have-Not Healthcare” marketplace patchwork.
What I had advocated back in late 2009 during the height of the “Healthcare Reform” debates was written into a position paper, “Rx for U.S. Healthcare Reform” (which you can click on the red-inked hyperlink to view in a new window or toggle to the bottom of his post to view an embedded “slide player” for reading or downloading). Out of this 23-page position paper, TANC (from the former advocacy group Trans-American Alliance for a National Consensus) explored an EXISTING quarter-century-old model for a tiny, "working" Medicare Advantage Part-D (MA-PD) program in which several "successsful," self-sustaining NONPROFIT-based "Social HMOs" for Seniors (like SCAN of California, Arizona and Nevada, Kaiser-Permanente and Eldercare of New York and New Jersey). All of these "no-to-low deductible" and "zero-to-minimal co-pay" MA-PD Social HMOs provided outstanding "nonprofit-based business models" of how to remove "profit exploitation" from healthcare as well as mitigate the corrosive "antitrust-exempt monopoly powers" of FOR-PROFIT/Big Health Insurance carriers.
In fact, by illustrating the broader abilities and scope of other "Nonprofit Community Health Plans" in about two-thirds of the states in America, the "working success" of MA-PD Social HMOs in the Senior marketplace provided the basis of broadening out "nonprofit-based healthcare" to under-65 patients/consumers.
Additionally, a single payer-based, "Medicare-for-All" universal access healthcare system as proposed by Sen. Sanders and other progressive advocates, does NOT have to "burden" LOW- to MIDDLE-INCOME TAXPAYERS with new large-scale "tax levies" to be fully funded: Our "Rx for U.S. Healthcare Reform" paper actually proposes a new "Federal Excise Tax on the Manufacturers of Unhealthy Consumable Products," such as cigarettes, alcoholic beverages, fast foods, sweetened beverages, candies, sugar-based confectionery baked goods, and packaged snack foods, etc. -- the makers of products that historically have placed the "biggest financial and physical burdens" on American health care systems.
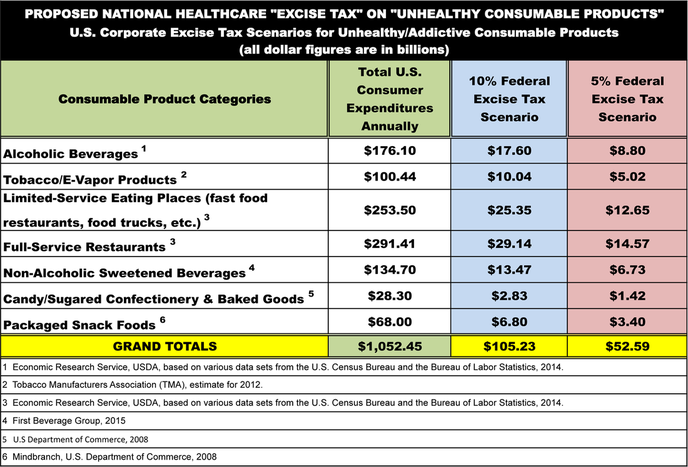
Our estimates are that a new EXCISE TAX on "unhealthy consumables" could raise between $50 billion to just over $100 billion annually – as proposed in the attached chart in either 5% or 10% excise scenarios -- in additional “National Healthcare Tax” revenues to help defray the costs of a "nonprofit-based" Single-Payer/Medicare-for-All healthcare system.
That, along with trying again to get Congress to repeal th 71-year-old "antitrust-exempt" monopoly powers status (from the McCarran-Ferguson Act of 1945) and a proposed "Federal Nonprofit Healthcare Conversion" bond issuing program would remove the overwhelmingly punitive "FOR-PROFIT EXPLOITATION" and Wall Street stock marketplace pressures on our long-standing "exclusionary" Have or Have-Not Healthcare patchwork.
Over 85 advanced countries have been offering various forms of "Universal Access" healthcare systems -- all of them with FAR cheaper, accessible and equitable healthcare that Americans have been saddled with from a punitive, artificially-overpriced and PROFIT-OBSESSED "middleman" Big Health Insurance MONOPOLY (please watch our embedded video presentation of PBS’s 5-nation exploration of Universal Healthcare systems in “Sick Around the World”).
Starting with the colonization of America in the 17th century, our country was founded on the basis of NONPROFIT-based community and ecumenical healthcare but near the turn of the 20th century "profit exploitation" took control of an exclusionary, punitive healthcare patchwork -- one which every major religious and civil rights leader (quoted in this position paper!) describes as being an AFFRONT to humanity, sacrifice and the divine right every American has to obtain proper healthcare!
Please give a read of this position paper and other supporting material when you can spare time, in addition to SHARING this post and position paper with every "Bernie Sanders"-related Facebook group and page, in addition with the Senators office. There are established "road maps" to NONPROFIT-BASED, universally-accessible and low- to no-cost healthcare! May good health and financial security be with you all (and away from going bankrupt by NOT being insured or under-insured) as a RIGHT for all Americans! #
– Michael A. Freeman

 RSS Feed
RSS Feed
